
ORIGINAL ARTICLE
FREQUENCY OF RADIAL ARTERY OCCLUSION IN PATIENTS UNDERGOING PERCUTANEOUS CARDIAC CATHETERIZATION BY RADIAL ACCESS
Usman Mahmood Butt1 , Muhammad Abu Bakar2 , Muhammad Khaleel Iqbal1 , Shahzad Shoukat3 , Rao Shahzad Abdul Tawwab Khan4 , Muzaffar Ali1
1Jinnah Hospital, Lahore, Pakistan, 2Faisalabad Institute of Cardiology, Faisalabad, Pakistan, 3Punjab Institute of Cardiology Lahore, Pakistan, 4Wazirabad Institute of Cardiology, Wazirabad, Pakistan
INTRODUCTION
The most common site used for percutaneous coronary intervention is femoral artery. This approach is troubled with risk of puncture site bleeding, which deteriorates the outcome of the patient, despite easiness and simplicity of this approach 2 In modern era alternative access through the radial artery is becoming more and more popular due to a substantial reduction of puncture site bleeding complication in comparison to femoral artery access. The recent ESC guidelines recommend radial access in ST-segment elevation myocardial infarction (STEMI) patients as a preferred approach in terms of reduction in primary outcomes like death, myocardial infarction and stroke. On top of that this approach provides comfort to the patient regarding mobility, short post catheterization stay at hospital and less financial burden on the patient. But the main problem with transradial approach (TRA) is radial artery occlusion (RAO) after the procedure.2-4
RAO is the commonest complications of cardiac catheterization performed through this approach (incidence 0.8%-30%). 5 In some other studies the overall incidence of RAO varies from 1.5 % to 30.5% (average 5-12 %).6,7 One study showed that there were only 9.4 % patients who has RAO after transradial catheterization.1 But another study showed that RAO was reported in 15.2% patients.8 After transradial procedures, hemostasis is secured either with elastic bandage application or using dedicated graded radial pressure devices. Such devices are usually applied to maintain patent hemostasis where distal flow via radial artery is not hampered during the process of hemostasis due to just adequate amount of pressure applied. Such dedicated devices, despite being the current standard of care in developed countries, are still not being use in local centers due to cost and availability issues. Most of the published data regarding radial artery occlusion rates after cardiac catheterization comes from the centers where dedicated graded radial pressure devices are standard of care. With locally practiced elastic bandage application, the amount of pressure can be adjusted. Thus, RAO is not uncommon finding rendering radial artery not useable for any further catheterization. Local data does not exist in this regard and the international data is quite variable and that too is with dedicated devices.
We intend to carry out this study in order to assess RAO rates in our local practice where elastic bandage is used for hemostasis. In case of high RAO rates, use of dedicated devices may be advocated for better patient care. Therefore; the present study was planned to assess the frequency of radial artery occlusion (RAO) in patients undergoing percutaneous cardiac catheterization.
METHODOLOGY
RESULTS
DISCUSSION
Radial artery occlusion (RAO) is the commonest complications of cardiac catheterization performed through transradial approach. In some studies the overall incidence of RAO varies from 1.5% to 30.5% (average 5-12 %).6 The incidence of RAO rests on various demographics, clinical and periprocedural factors, along with the time passed from the procedure to the radial artery examination for patency. This incidence further decreases by 50% if the radial artery is examined 30 days after cardiac catheterization, as compared to the instant checkup of the radial artery after the removal of pressure bandage removal. It reveals spontaneous radial artery recanalization.9,10
In our study it was intended to measure the frequency of radial artery occlusion through transradial approach in our population as local data is lacking and transradial access is less commonly approached regardless of its well-known safety and efficacy.
In our study the patients who underwent percutaneous cardiac catheterization via the transradial approach were present with the mean age of 52.56 ± 11.86 years which is similar to a study by Masud F et al. documenting mean age of 57.62 ± 10.1 years.11 Another study by Chowdhury MZ reported the mean age of patients 53.5 ± 9.7 years (range: 31-75 years) which is similar but, in this study, when data was categorized in the groups it was seen that the most of the patients had age more than 50 but statistically insignificant difference was observed among age groups. In contrast to our results aforementioned studies reported age as a prognosticator of RAO, with elderly patients (above 60 years) having higher frequency of RAO. Similarly, 63.8% with age >50 years were declared to be having RAO by Chowdhury.12 Male into female percentage in our study was perceived to 63.4% versus 36.6% which is in line with the literature showed two thirds (66.7%) were male by Chowdhury. Another study reported comparable results with respect to gender (male 68.8% and female 32.2%).
All patients were overweight and obese in our results who present for PCI whereas the normal weight patients (47.8%) were also foreseen in previous studies incidence of overweight and obese patients was 43.5% and 8.7% respectively. Incidence of hypertension, diabetes mellitus (DM), dyslipidemia and smoking were 80%, 65%, 57% and 38% respectively.12 A Study by Tuncez had inverse results with respect to high percentage of female gender (56.6%) and Hypertension (81.1%) DM (34.9%) Hyperlipidemia (85%) Smoking (47.2%).1
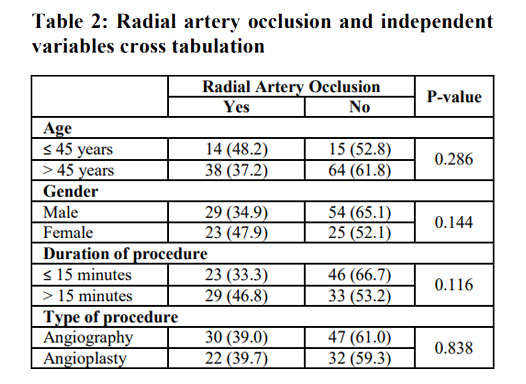
When data was stratified with respect to effect modifiers it was noted that among age, gender, duration of procedure or type of intervention; statistically insignificant difference was observed among the radial artery occlusion and these variables. In the previous data, there was significant variation in RAO frequency in stratification of data for gender. A study by Masud F et al. conducted on 141 patients, RAO was found in 10 (7.1%) patients and out of these 6 (60%) were females and 4 (40%) were males.11 Similar trends were seen in studies done by Tuncez et al. (80 % female patients with RAO) and Rashid et al. (66.7% female patients with RAO). This gender difference is most probably due to main factor of small ration of radial artery to arterial sheath seen in females.14 A local study demonstrated that higher incidence of RAO was seen in patients undergoing PCI (9) as compared to those undergoing angiogram (1) and these results were in accordance to study by Tuncez et al. In those 10 patients with RAO there was difference of procedure time (<30 min in 1, <60 min in 7 and >1-hour in 2 patients). But the effects of procedure type and duration on RAO were not statistically significant (p-value=0.195 and 3.55).11 Sinha study results provided multivariate analysis, and prove that various predictors of RAO include female gender, DM, low BMI, small radial artery (≤2.2 mm) and small radial artery to sheath ratio < 1. 16

Mean interval of Cine-fluoroscopy for coronary angiography was 2.75 ± 1.5 min and percutaneous coronary intervention (PCI) 8.29 ± 5.1 minutes. 1 These results are in accordance to previous data. Whereas in our study duration of coronary angiography by radial artery is 18.22 minutes and PCI 19.24 minutes.
The frequency of RAO was found to be 39.7% in our study and in another study, this was 7.1%11 which is less than in comparison to a large study by Tuncez et al. (9.4%).1 In another study by Indian Sreevasta et al. it was 13.1%. 13 These findings are in accordance to current meta-analysis published by Rashid et al. where RAO incidence was found to be 7.7% in first 24 hours and 5.8% after 30 days of cardiac catherization.14
In contrast to above mentioned results related to incidence of RAO, study by Chowdhury done on 69 patients undergoing cardiac catheterization, only one old age patient (1.45%) had RAO on follow-up at third month which is quite less than documented (up to 18%) by some other studies.1-7 Although this patient was asymptomatic despite ischemic hand detected by no radial artery flow on Doppler ultrasound (USG), which could be explained by the presence of collaterals. Therefore, Kiemeneij recommended that radial approach for cardiac catheterization should be selected only in those patients with good ulnar and palmar arch blood flow.15 The patency of these vessels can be checked by the Allen’s test before starting the procedure but gold standard methods are color doppler USG and plethysmography.12
Sinha et al. 16 study 1945 consecutive patients undergone transradial catheterization demonstrated that RAO was found in 339 (174%) patients through color doppler USG on day 1, although pulse was still palpable on examination in 115 (34%) of these patients. While 30-day data showed RAO was found in 221 (11.4%) patients and 114 (52%) patients had palpable pulse. Surprisingly, 118 (34.8%) of 339 patients having RAO showed spontaneous recanalization of the radial artery on doppler USG. Further follow up on 180 days, there was reduction in RAO to 99 (5.1%) and palpable radial artery in 68 (69%) patients was found which indicated more spontaneous recanalization.16
In our study there was significant reduction in RAO at 30 day by compressing ipsilateral ulnar artery prophylactically during radial artery compression for hemostasis after catheterization through radial approach. Rather RAO was and indeed, we found that the incidence of RAO was reduced after 1 week compared with the day of the procedure.
CONCLUSION
AUTHORS' CONTRIBUTION
REFERENCES
2. Bernat I, Aminian A, Pancholy S, Mamas M, Gaudino M, Nolan J, et al. Best Practices for the Prevention of Radial Artery Occlusion After Transradial Diagnostic Angiography and Intervention: An International Consensus Paper. JACC Cardiovasc Interv. 2019;12(22):2235-46.
3. Slawin J, Kubler P, Sczezepanski A, Piatek , Stepkowski M, Reczuch K. Radial artery occlusion after percutaneous coronary interventions an underestimated issue. Postepy Kardiol Interwencyjnej. 2013;9:353-61.
4. Pancholy SB, Bernat I, Bertrand OF, Patel TM. Prevention of Radial Artery Occlusion After Transradial Catheterization: The PROPHET-II Randomized Trial. JACC Cardiovasc Interv. 2016;9(19):1992-99.
5. Wagener JF, Rao SV. Radial artery occlusion after transradial approach to cardiac catherization. Curr Atheroscler Rep. 2015;17:1-8.
6. Bertrand OF, Rao SV, Pancholy S, Jolly SS, Rodes-Caban J, Larose E, et al. Transradial approach for coronary angiography and interventions: results of the first international transradial practice survey. J Am Coll Cardiol Cardiovasc Interven. 2010;3:1022-31.
7. Lavi S, Cheema A, Yadegari A, Israeli Z, Levi Y, Wall S, et al. Randomized trial of compression duration after transradial cardiac catheterization and intervention. J Am Heart Assoc. 2017;6(2):e005029.
8. Garg N, Madan B.K, Khanna R, Sinha A, Kapoor A, Tewari S, et al. Incidence and Predictors of Radial Artery Occlusion After Transradial Coronary Angioplasty: Doppler-Guided Follow-up Study. J Inv Cardio. 2015;27(2):106-12.
9. Ali S, Abdullah MS, Abdelrahman K, Ali A, Faisal F, Ali A. Total Radial Artery Occlusion Following Transradial Access: Complete Recanalization via the Anatomical Snuffbox. Methodist Debakey Cardiovasc J. 2020;16(4):314-7.
10. Koutouzis M, Maniotis C, Avdikos G. Prevention of Radial Artery Occlusion After Transradial Catheterization. JACC Cardiovasc Interv. 2017;10(1):103.
11. Masud F, Hassan Y. Radial artery occlusion- a burden or a challenge? Pak Heart J. 2017;50(01):14-8.
12. Chowdhury MZ, Kabir CMS, Nasrin S, Gomes HI, Hakim E, Khan SR, et al. Radial Artery Patency after Trans-radial Cardiac Catheterization in a Bangladeshi Population. Uni Heart J. 2014; 10(2):66-72.
13. Tewari S, Sharma N, Kapoor A, Syal SK, Kumar S, Garg N, et al. Comparison of transradial and transfemoral artery approach for percutaneous coronary angiography and angioplasty: aretrospective sevenyear experience from a north Indian center. Indian Heart J. 2013;65(4):378-87.
14. Rashid M, kwok CH, Pancholy S, Chugh S, Sasko A, Ratib K, et al. Radial artery occlusion after transradial Interventions: a systemic review and meta-analysis. J Am Heart Assoc. 2016;5(1):26-86.
15. Hahalis G, Aznaouridis K, Tsigkas G, Davlouros P, Xanthopoulou I, Koutsogiannis N, et al. Radial Artery and Ulnar Artery Occlusions Following Coronary Procedures and the Impact of Anticoagulation: ARTEMIS (Radial and Ulnar ARTEry Occlusion Meta-AnalysIS) Systematic Review and MetaAnalysis. J Am Heart Assoc. 2017;6(8):e005430.
16. Sinha SK, Jha MJ, Mishra V, Thakur R, Goel A, Kumar AA. Radial Artery Occlusion – Incidence, Predictors and Long-term outcome after TRAnsradial Catheterization: clinico-Doppler ultrasound-based study (RAIL-TRAC study). J Acta Cardiologica 2017;72(3):318-27.
Address for Correspondence:
Email: usman_sw@hotmail.com