
ORIGINAL ARTICLE
EVALUATION OF THE QUANTITY AND DURATION OF JUNCTIONAL RHYTHM DURING SUCCESSFUL RADIOFREQUENCY ABLATION AMONG PATIENTS WITH ATRIOVENTRICULAR NODAL RE-ENTRY TACHYCARDIA
Usman Mahmood Butt1 , Imran Saleem1 , Hafiz Abdul Mannan Shahid1 , Waqar Hassan1 , Muhammad Ashraf Dar1 , Zubair Akram2
1Punjab Institute of Cardiology, Lahore, Pakistan, 2Allama Iqbal Medical College/Jinnah Hospital, Lahore, Pakistan
INTRODUCTION
Among supraventricular tachycardia (SVT), atrioventricular nodal reentrant tachycardia (AVNRT) is the commonest of all. The AVNRT includes an extra pathway in the atrio-ventricular node (AV node) that takes part in the reentry circuit.1 This is the most common mechanism in around 60% of the patients who present with the history of supraventricular tachycardia.2
Regarding treatment of AVNRT, the most effect way is the radiofrequency ablation (RFA) of the slow pathway for its permanent termination. This RFA of the slow pathway is directed by combined information from fluoroscopic imaging, intra-cardiac electrograms pattern and the initiation of junctional rhythm (JR) during energy delivery.3 During RFA of the slow pathway, the initiation of junctional rhythm is a wellamong AVRNT patients although during RFA of slow pathway, the occurrence of junctional rhythm is a well-documented indicator of successful treatment of AVNRT and it is necessary to evaluate the amount and duration of accelerated junctional rhythm during RFA in our population.
METHODOLOGY
DISCUSSION
Junctional rhythm (JR) may be used as an indicator of success in the treatment of AVNRT through RFA of slow pathway. RF energy should not be delivered if JR does not appear within first 20 seconds of start of ablation.8 In our study while RFA at successful anatomic studies, although this is not related to increasing age.14,20
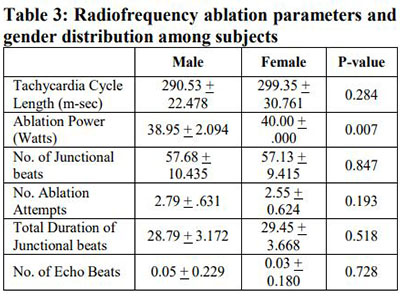
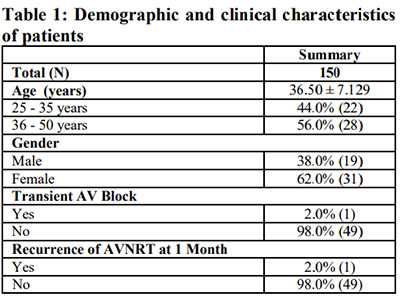
The existence of residual slow pathway in the form of AV nodal Echo beats after RFA is considered to be related to recurrence of AVNRT. An important indicator of residual slow pathway after RFA of slow pathway is the presence of AV nodal Echo found in many studies.14, . 15 Similarly in our study only 2 patients (out of total 50) showed AV nodal echo beat and only 1 patient showed recurrence of AVNRT at 1 month. In another study by Nikoo MH et al, the endpoint of RFA is either slow pathway ablation or modification with only 1 AV nodal echo beat post ablation.16 Wagshal et al, studied various forms of junctional rhythm during slow pathway ablation, they found that higher temperature during ablation resulted in higher success rate in abolition of slow pathway but there was shorter duration and number of accelerated junctional beats. They found that the junctional rhythm was specific for slow pathway in AV node.17 A study done by Abdel Motelb showed 100% of patients had junctional rhythm while ablation at the successful sites. It was seen that JR was highly sensitive predictor of effective ablation but not so specific marker (60%). Almost six patterns of JR were detected.7 Our study also compared different parameters and ablation power was statistically significant among gender. (p < .05).
Safety of an invasive is an important aspect as shown by the study of DG et al, there were vascular complications and transient AV block in around 0.3%. of patients.11 Chrispin et al, did study on RFA of slow pathway in AVNRT which showed transient AV block in around 0.4% of patients.8 These results were in accordance to our study regarding transient AV block during procedure which was improved at 1 month follow up. In a study conducted by Ahmad et al, showed similar results of successful ablation of AVNRT in terms of non-inducibility of clinical tachycardia in 59.4% of patents and development of JR in 80.8% of patients with high specificity of 89.6%.18
RFA of slow pathway is also safe and effective in AVNRT patients of pediatric age group. But there is need of further research in this age group to establish endpoints of ablation and risk factors for the recurrence of AVNRT. 19 Given the very high success rates (approximately 98%) for catheter ablation in AVNRT, this procedure is considered the treatment of choice. During this procedure, the SP is targeted, using either radiofrequency energy or cryoablation, with the aim of rendering the tachycardia non-inducible at the end of the procedure.21
7. Abdel Moteleb AM, Khalid SA, Ibrahim MM. Junctional rhythm occurring during AV nodal reentrant tachycardia ablation, is it different among Egyptian. Egypt Heart J. 2013;65(4);265-70
8. Chrispin J, Misra S, Marine, J.E, Rickard J. Kolandaivelum BA, Ashikaga H et al. Current management and clinical outcomes for catheter ablation of atrioventricular nodal re-entrant tachycardia Eur Heart J. 2018;20:e51-e59
9. Ding L, Weng S, Zhang H, Fengyuan Yu, Yingjie Qi, Zhang S, et al. Slow-Pathway Visualization by Using Panoramic View: A Novel Ablation Technique for Ablation of Atrioventricular Nodal Reentrant Tachycardia. J Cardiovasc Dev Dis. 2022;9(4):9.
10. Katritsis DG, Zografos T, Siontis KC, Giannopoulos G, Muthalaly RG, Liu Q et al. Endpoints for Successful Slow Pathway Catheter Ablation in Typical and Atypical Atrioventricular Nodal ReEntrant Tachycardia: A Contemporary, Multicenter Study. JACC Clin Electrophysiol. 2019;5(1):113-9.
11. Thibault B, de Bakker JM, Hocini M, Loh P, Wittkampf FH, Janse MJ. Origin of heat-induced accelerated junctional rhythm. J Cardiovasc Electrophysiol. 1998;9(6):631-41.
12. Jentzer JH, Goyal R, Williamson BD, Man KC, Niebauer M, Daoud E, et al. Analysis of junctional ectopy during radiofrequency ablation of the slow pathway in patients with atrioventricular nodal reentrant tachycardia. Circulation. 1994;90:2820-6
13. Hale ZD, Greet BD, Burkland DA, Greenberg S, Razavi M, Rasekh A, et al. Slow-pathway visualization by using voltage-time relationship: A novel technique for identification and fluoroless ablation of atrioventricular nodal reentrant tachycardia. J Cardiovasc Electrophysiol. 2020;31(6):1430-5.
14. Felix K, WegnerMS, Maria S, Bögeholz N, Leitz PR. Slow pathway modification in patients presenting with only two consecutive AV nodal echo beats. Cardiol J. 2017;69(2):471-5.
15. Manolis AS, Maounis T, Vassilikos V, Chiladakis J, Cokkinos DV. Arrhythmia recurrences are rare when the site of radiofrequency ablation of the slow pathway is medial or anterior to the coronary sinus os. Europace. 2002;4(2):193-9.
known indicator of success in the treatment of AVNRT.4 Ablating the slow pathway (SP) is the superior treatment for atrioventricular nodal reentrant tachycardia (AVNRT) with a low complication rate. However, the ablation of the SP could result in either complete elimination or modification of the SP.5
A study conducted by Iakobishvili et al, during successful RFA of the slow pathway total number of junctional beats varied from 3 to 226 (mean 37 ± 12), while in ineffective RFA these beats were between 3 to 33 (mean 15 ± 2; p=0.01).6 In another study by Abdel Moteleb et al, during successful RFA of the slow pathway the duration of JR varied from 1.1- 113 sec (mean 19.1 ± 21.3 sec), while in ineffective RFA this duration was between 1.5-18 sec (mean 8.5 ± 7.3 sec; p=0.01).7
We aim to evaluate the quantity and duration of junctional rhythm during radiofrequency ablation In case of recurrent symptoms further testing like holter monitoring done if required. SPSS software version 21.0 was used for statistical analysis. For the calculation of normally distributed parameters descriptive statistics in terms of mean ± SD were used. While for skewed parameters median and interquartile range were used. Independent t test was applied to assess statistical significance for number and duration of junctional beats in successful and unsuccessful ablation with p < .05 as statistical significance.
RESULTS
ablation site resulted in induction of junctional rhythm in all the patients included in the study (100%). These trends are in accordance with other studies that show the occurrence of junctional ectopic beats during RFA of slow pathway in patients with AVNRT. This junctional ectopic rhythm during RF of slow pathway is a sensitive but non-specific predictor of success.9
In a study by Katritsis et al, the absence of AVNRT at 3 months following RFA, which resulted in induction of junctional rhythm had high sensitivity of around 95.9% (94.6% to 97.0%) while specificity was 4.20% (0.11% to 21.10%).10 There are several hypothesis of this junctional ectopic rhythm during RFA of slow pathway like presence of heat sensitive region compact AV node and increase release of noradrenaline form post sympathetic nerve endings.11
The results of our study are similar to Jentzer et al study on RFA of slow pathway for the treatment of AVNRT. The study included 50 consecutive patients of AVNRT who undertook RFA of slow pathway and another 5 patients were added in the study retrospectively due to development atrioventricular (AV) block during RFA. The occurrence of JR was statistically significant during effective RFA as compared to 366 ineffective RFA attempts (100% vs 65%, P < .001). Similarly effective RFA attempts had a significantly longer duration of junctional ectopic beats as compared to non-effective attempts.12
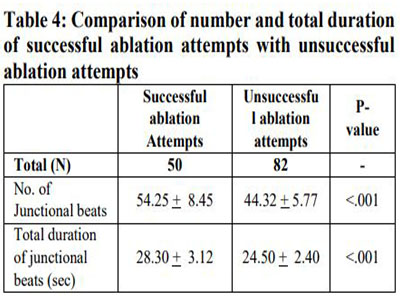
When compared unsuccessful RFA with, successful RFA there was significantly longer duration of junctional beats in this group (19 ± 15 vs 11 ± 12 s, P < .01). In our study incidence of junctional beats was statistically high in successful ablation attempts group as compared to unsuccessful attempts group (54.25 + 8.45 vs 44.32 + 5.77 p value= .000). Similarly total duration of junctional beats was statistically high in successful ablation attempts group as compared to unsuccessful attempts group (28.30 + 3.12 vs 24.50 + 2.40 p value= .000). This was major finding of our study that in successful ablation attempts group there was there was greater amount and duration of junctional beats as compared to unsuccessful group. Although the achievement of ⩾1 JR was necessary to obtain the non-inducibility, and the cumulative number of junctional beats (CJB) was higher in effective applications, no CJB cut-off was associated with a success rate higher than 75%.7 In another study by Hale ZD et al, the occurrence of Junctional rhythm was present in 40/41 RFA (98%) at the expected site of slow pathway in AV node.13 In our study50/50 RFA (100%) at slow pathway showed junctional rhythm. Significant variability in the location of the SP and the anatomy of the triangle of Koch has been demonstrated using electroanatomic mapping and Our study has several limitations. Firstly, this was a study done in a single center with small sample size. A multicenter prospective study with larger sample size should be done to validate these results of safety and efficacy of RFA and to see the results of these procedures in atypical AVNRT. To be more precise panoramic view (PANO) could have been used for slow-pathway localization. And lastly elderly patients of age more than 50 years should be included to look for influence of age on the anatomy of slow-pathway as they have high risk of AV blocks.
CONCLUSION
AUTHORS' CONTRIBUTION
UMB and IS: Concept and design, data acquisition, interpretation, drafting, final approval, and agree to be accountable for all aspects of the work. HAMS, WH, MAD, and ZA: Data acquisition, interpretation, drafting, final approval
Conflict of interest: Authors declared no conflict of interest.
REFERENCES
2. Kotadia ID, William SE, Neil M. Supraventricular tachycardia: An overview of diagnosis and management. Clin Med (Lond). 2020;20(1):43-7.
3. Bagherzadeh A, Rezaee ME, Farahani MM. Prediction of Primary Slow-Pathway Ablation Success Rate according to the Characteristics of Junctional Rhythm Developed during the Radiofrequency Catheter Ablation of Atrioventricular Nodal Reentrant Tachycardia. JTHC. 2011;6(1):14-8.
4. Sugumar H, Chieng D, Prabhu S, Voskoboinik A, Anderson RD, Al-Kaisey A, et al. A prospective evaluation of the impact of individual RF applications for slow pathway ablation for AVNRT: Markers of acute success. J Cardiovasc Electrophysiol. 2021;32(7):1886-93.
5. Raharjo SB, Togatorop BT, Andriantoro H, Hanafy DA, Yuniadi Y. AH jump duration is associated with elimination of slow pathway during ablation of atrioventricular nodal reentrant tachycardia. IPEJ. 2020;20(4):160-3.
7. Abdel Moteleb AM, Khalid SA, Ibrahim MM. Junctional rhythm occurring during AV nodal reentrant tachycardia ablation, is it different among Egyptian. Egypt Heart J. 2013;65(4);265-70
8. Chrispin J, Misra S, Marine, J.E, Rickard J. Kolandaivelum BA, Ashikaga H et al. Current management and clinical outcomes for catheter ablation of atrioventricular nodal re-entrant tachycardia Eur Heart J. 2018;20:e51-e59
9. Ding L, Weng S, Zhang H, Fengyuan Yu, Yingjie Qi, Zhang S, et al. Slow-Pathway Visualization by Using Panoramic View: A Novel Ablation Technique for Ablation of Atrioventricular Nodal Reentrant Tachycardia. J Cardiovasc Dev Dis. 2022;9(4):9.
10. Katritsis DG, Zografos T, Siontis KC, Giannopoulos G, Muthalaly RG, Liu Q et al. Endpoints for Successful Slow Pathway Catheter Ablation in Typical and Atypical Atrioventricular Nodal ReEntrant Tachycardia: A Contemporary, Multicenter Study. JACC Clin Electrophysiol. 2019;5(1):113-9.
11. Thibault B, de Bakker JM, Hocini M, Loh P, Wittkampf FH, Janse MJ. Origin of heat-induced accelerated junctional rhythm. J Cardiovasc Electrophysiol. 1998;9(6):631-41.
12. Jentzer JH, Goyal R, Williamson BD, Man KC, Niebauer M, Daoud E, et al. Analysis of junctional ectopy during radiofrequency ablation of the slow pathway in patients with atrioventricular nodal reentrant tachycardia. Circulation. 1994;90:2820-6
13. Hale ZD, Greet BD, Burkland DA, Greenberg S, Razavi M, Rasekh A, et al. Slow-pathway visualization by using voltage-time relationship: A novel technique for identification and fluoroless ablation of atrioventricular nodal reentrant tachycardia. J Cardiovasc Electrophysiol. 2020;31(6):1430-5.
14. Felix K, WegnerMS, Maria S, Bögeholz N, Leitz PR. Slow pathway modification in patients presenting with only two consecutive AV nodal echo beats. Cardiol J. 2017;69(2):471-5.
15. Manolis AS, Maounis T, Vassilikos V, Chiladakis J, Cokkinos DV. Arrhythmia recurrences are rare when the site of radiofrequency ablation of the slow pathway is medial or anterior to the coronary sinus os. Europace. 2002;4(2):193-9.
17. Wagshal AB, Crystal E, Katz A. Patterns of accelerated junctional rhythm during slow pathway catheter ablation for atrioventricular nodal reentrant tachycardia: temperature dependence, prognostic value, and insights into the nature of the slow pathway J Cardiovasc Electrophysiol. 2000;11:244-54.
18. Ahmad S, Khan A, Ullah I. Success rate in patients with atrioventricular nodular re-entrant tachycarida (AVNRT) slow pathway catheter ablation with and without junctional rythym. PJMHS. 2022;16(11):626-8.
19. Hayun MC. RFCA is safe and effective in pediatric AVNRT patients. However, further research is needed for establishing the endpoints of ablation in pediatric AVNRT patients and for identifying risk factors by evaluating data on AVNRT recurrence after RFCA. Clin Exp Pediatr. 2017;60(12):390-4.
20. Hong KL, Verma A, Lee T, Jiang Y, Skobic D, Huang G, et al. Age-Related changes in the anatomy of the triangle of koch: Implications for catheter ablation of atrioventricular nodal re-entry tachycardia. CJC Open. 2021;3:924-8.
21. Ector J, Haemers P, Garweg C, Willems R. Diagnosis and treatment of atrioventricular nodal reentrant tachycardia: a case report illustrating clinical management and ablation strategy. Eur Heart J Case Rep. 2020;4(4):1-7.
Address for Correspondence:
Email: usman_sw@hotmail.com